Safety Alert
Nature Medicine - AI Section⭐Promising2 min read
Genetic testing spots future tumor risks in children
Key Takeaway:
Identifying inherited cancer-risk genes in pediatric patients helps doctors predict future tumor risks, allowing for personalized long-term monitoring and counseling starting today.
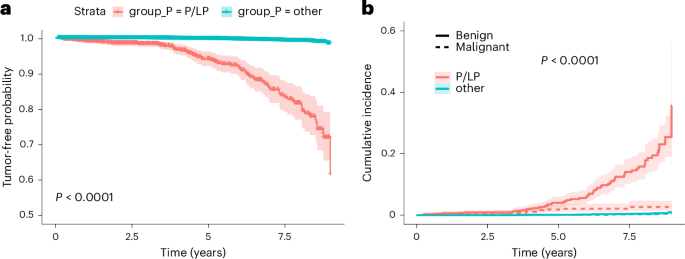
A peer-reviewed study published in Nature Medicine analyzed large-scale genomic data from pediatric patients referred for genetic testing. Researchers discovered a statistically significant link between inherited gene mutations and the subsequent development of tumors. By tracking these genetic markers over time, the study proves that inherited risk genes can reliably predict future cancer events in children. This finding is crucial because it gives pediatricians a clear roadmap to start personalized long-term monitoring and counseling early, potentially catching and treating tumors before they become life-threatening.
What this means for you
This study shows that genetic testing can identify children with a higher risk of developing future tumors. Talk to your doctor about genetic counseling, but do not alter current medical care.
Citation:
Nature Medicine - AI Section, 2026. DOI: s41591-026-04451-1 Read article →